
What I Heard, and What It's Costing You
You started as eight providers, small enough that one person saw every inquiry that came in. You tripled through the pandemic, went all-telehealth, then hybrid, and today you run 80 clinicians across five locations. The systems that worked at eight didn't scale with you. They got patched and worked around. That gap is where the money is leaking.
You said it plainly on our call, and it was the clearest statement of the problem anyone made:
"When we were smaller, we used to be able to fill all our openings in a given week. And as we got larger, we have not been able to do that. We're losing money by not filling those slots earlier." Dr. Barbara Brown
Here's what happens to a new client today, start to finish:
- An inquiry comes in by phone, website, or email. Around 200 calls a week land across billing, front desk, and intake. Only about 25 a week come through website scheduling.
- On a live call, an intake person spends roughly 15 minutes matching the client to a clinician by insurance, specialty, location, availability, and supervisor rules.
- If they can't be placed live (wrong insurance, no fit, or not enough time on the call), they get added by hand to a waitlist that's been living in Excel.
- Phone-placed clients skip the website form flow. Staff set up their portal, email them, then send forms through the portal.
- The client doesn't fill the forms out, so your team follows up. And follows up again.
- Insurance cards and credit cards can't be required up front, so each one turns into another email and another wait.
- A triage flag, where a client screens positive for crisis, hard-stops the whole flow until a clinician can be pulled onto a call.
- By the time the loop closes, the same-week slot is gone. The appointment slides a week or two out, and sometimes the client is gone with it.
Every step there is a spot where a client who was ready to book can stall out and go cold. The leak is worst at the exact moment they're most likely to commit.
When I asked where it actually breaks, you didn't hesitate:
"The broken part is the conversion between the call and the scheduling." Dr. Barbara Brown
What this is really costing you
- Unfilled slots. Every same-week opening that slides a week is revenue you had the demand for and didn't capture. Across 80 clinicians, a few unfilled slots each per week adds up fast. Quantifying it is one of the first jobs of discovery.
- Labor on follow-up. About 12 people across front desk, intake, and billing spend hours chasing forms, cards, and callbacks. Repetitive, rule-based work, which is exactly what automates well.
- Missed calls. Your phone went unanswered three times in a row on a test call. A missed call in mental health is often a client lost for good.
- Billing leakage. Note-to-claim mismatches like place of service or session length force a human to check every claim before it goes out. Denials, payments held past the 30-day requirement, and insurer AI audits are tracked by hand, if at all.
- A growth ceiling. Every one of these is people-heavy. The only way to grow it today is to hire more people, the exact cost you're trying to escape.
And this is happening while the ground shifts under you. You told me insurance is getting worse, that DOGE cuts pushed people off coverage and deductibles up, and that you need to diversify into subscription, concierge, employer, and government-contract revenue. Whatever gets built has to bend with that instead of breaking.
"I'd like to see everything connected to one system, whether they call or email or go on the website, so that it can all be handled immediately." Dr. Barbara Brown
Right instinct. It's also why this has to be mapped before it's built.
Why This Isn't Simple
The hard part isn't building any one automation. It's that you have a dozen real opportunities tangled together, and picking the wrong one to build first is an expensive mistake. That's the main reason quoting a fixed build right now would be irresponsible.
Across two calls you raised intake, new-patient scheduling, existing-client rescheduling, an AI voice agent, call monitoring, billing and note-to-claim sync, denial tracking, clearinghouse-to-bank reconciliation, bookkeeping, a marketing and SEO strategy remap, a custom mobile app, payer diversification, and a possible phone-system replacement. Every one is a legitimate build. They are not equally valuable and they are not equally feasible. The job of discovery is to find the one that combines the highest impact with the fastest path to working, so the first thing you ship pays for the rest.
This isn't marketing automation for a gym. Every channel that touches a client carries protected health information, which rules out most off-the-shelf chat and automation tools the moment patient data enters them. The right engine here is self-hosted (n8n on your own HIPAA-compliant cloud, under a BAA) so data never leaves infrastructure you control. Triage raises the stakes further. A crisis flag can't be left to AI judgment. It has to be deterministic, rule-based, and escalate to a human instantly. Getting that wrong isn't a bug, it's a liability.
Almost every option above depends on one unknown: how open InSync's API actually is. Can it be triggered to send portal messages and forms? Can data be written back, not just read? Can the external scheduler be wrapped or bypassed? You can get data in and out of InSync, but the exact limits decide what's automatable now versus what needs a workaround. A formal API audit is step one, and it changes the entire roadmap.
Scheduling is the obvious example. It isn't "find the next open slot." Each clinician takes different insurance plans, and some can't run a first appointment without a supervisor, so matching runs on insurance by specialty by location by availability by supervision rules. But the same holds across the business. Your triage screening, your billing and place-of-service rules, your denial handling, and your payer logic each carry their own real-world exceptions. AI can follow rules like these, but only once they're written down explicitly. Capturing that logic accurately, in your words, is a big part of what discovery is for.
Your move toward subscription, concierge, employer, and government-contract payers means any billing or scheduling architecture built rigidly today breaks the moment your model shifts. Designing for that flexibility is a decision that has to be made up front, not retrofitted later.
Where Clients Slip Through Today
Your current intake and billing path, with the leak points marked. Closing these gaps is what the blueprints are for.
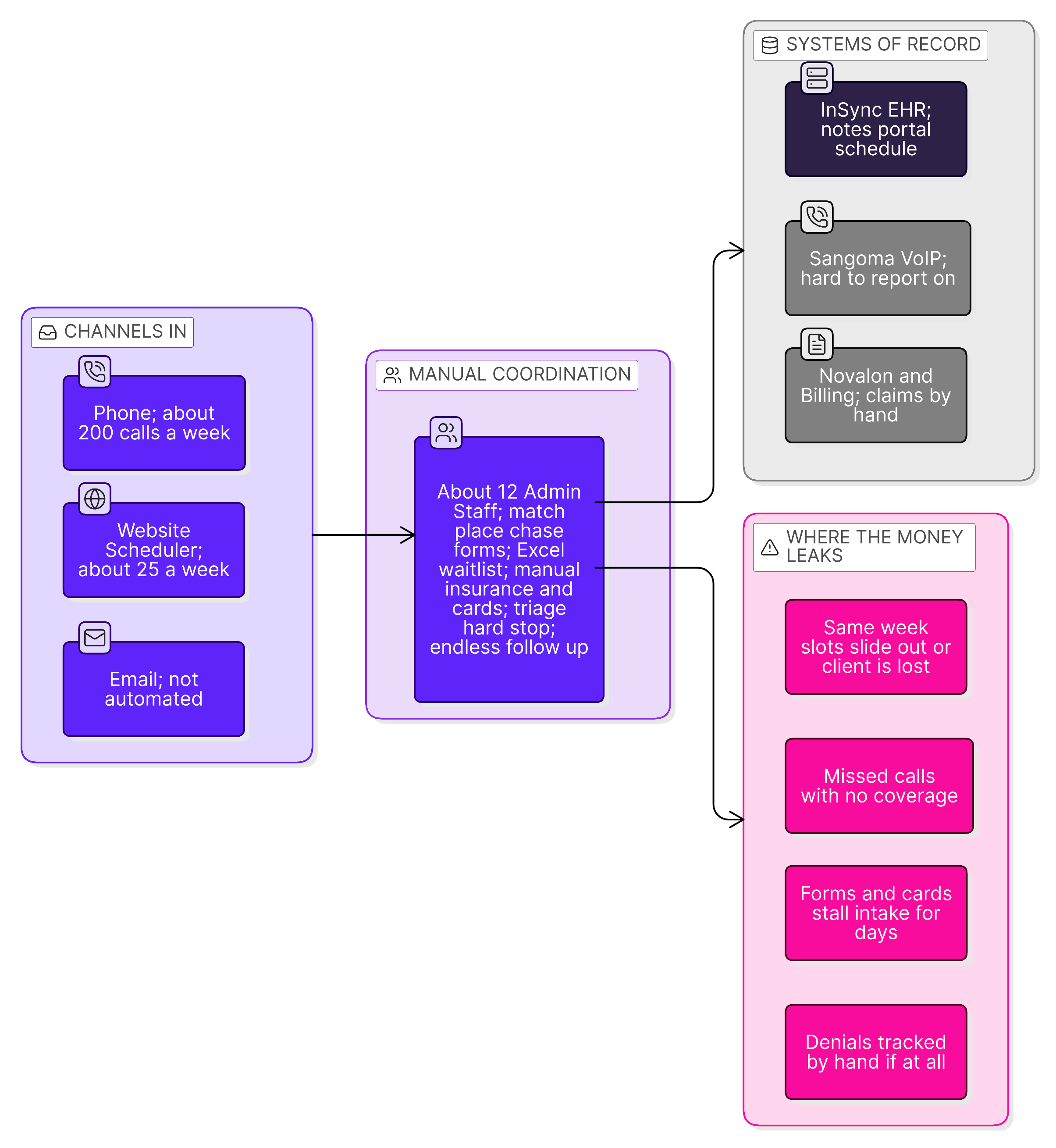
Current state. Gray arrows are today's manual handoffs. Pink marks the leak points discovery will quantify. There's no shared automation layer between these systems yet, which is the core of the opportunity.
What I'm Proposing
The leading hypothesis
Everything points to the conversion from first contact to booked appointment as your biggest single win. You diagnosed it yourself. The catch is that top of funnel is probably also the hardest part of your business to automate, because of the patient data, the triage liability, and the limits of the InSync API.
So the audit does two things at once. It designs the top-of-funnel fix properly, and it hunts for faster wins elsewhere, like billing and reconciliation, that we can ship while the bigger build gets planned. If your numbers point somewhere else entirely, we follow them.
What you get
- A full audit report of your operation and tech stack, including the HIPAA review and what the InSync API can and can't do.
- Three system blueprints, each with a detailed architecture diagram, the recommended tech stack, and the logic shell for how it runs. Some of the finer logic gets locked down during the build, not now, and the blueprint says clearly what's settled and what isn't.
- A prioritized ROI roadmap: what to build first, in what order, scored on impact and feasibility.
- A locked build price for each of the three systems.
- Up to 6 working calls with members of your team during the engagement.
The three blueprints
The two strongest are clear from our calls. Discovery confirms the third.
Omnichannel intake across phone, web, and email into one flow: insurance pre-check, clinician matching, triage escalation, and booking written back to InSync. A 24/7 AI voice agent so calls stop going unanswered. Aimed straight at the call-to-schedule gap and the empty same-week slots.
Note-to-claim checking before claims go out, denial and held-payment tracking, and clearinghouse-to-QuickBooks-to-bank reconciliation. This is close cousin to the River Oaks system I already built, designed here to flex as you add subscription, concierge, employer, and government payers.
The third comes from the next tier of value: AI voice plus call-quality and staff productivity monitoring, a marketing and SEO strategy remap, or a custom HIPAA mobile app with client self-scheduling and clinician rescheduling. We pick based on impact and your input.
What's not in this phase
Nothing gets built during discovery. This phase decides what to build and proves it before a dollar goes toward construction. It's also not a generic AI strategy deck. Every recommendation is grounded in your actual systems, your real API limits, and your own numbers.
Timeline & What I Need From You
| Stage | Focus |
|---|---|
| Days 1–4 | Kickoff. System access. InSync API audit. Map intake, scheduling, and phone flows with your team. |
| Days 5–10 | Map billing, denials, clearinghouse-to-bank, bookkeeping, marketing, and the payer-diversification plan. Quantify the slot-fill and follow-up costs. |
| Days 11–16 | Score every opportunity. Design the three blueprints. Lock each build price. |
| Wrap-up | Deliver the blueprints, the roadmap, and a walkthrough call. |
2-3 weeks of active work. The window depends on how fast access and answers come back. The timeline starts at the kickoff call, not the date of agreement.
What I need from you
- Read access to the systems you can share: InSync, the website scheduler, the clearinghouse view, QuickBooks, and the phone system.
- A point of contact for the InSync API, their support or your account rep, so the API audit isn't blocked.
- Short working calls with Kait, Jess, and whoever owns billing. For the phone-system review, a collaborative framing to William so it lands as cooperation rather than a turf war.
- Responses within 24 to 48 hours during the engagement. The faster access flows, the faster this lands.
One note on scope: I'm an automation and systems specialist, not a legal or HIPAA compliance authority. The blueprints will flag compliance considerations clearly, and final compliance sign-off stays with you and your counsel.
Investment
The second half is invoiced once the blueprints and roadmap are in your hands. Platform or hosting costs for a future build, like the self-hosted automation engine, are itemized inside the blueprints and paid directly to providers, never to me.
The bottom line
Across 80 clinicians, recovering even a handful of those unfilled slots per week pays for this engagement many times over in the first month, before the labor you save on follow-up or the calls you stop missing. And you keep three build-ready system designs you could hand to a developer tomorrow. Discovery is the cheapest way to make sure your build money goes to the thing that actually moves the number.
Your risk on this is close to zero
The second half doesn't get invoiced until the blueprints and roadmap are in your hands. If they're not, you don't owe it. And whatever happens, the work is yours to keep: take it in-house or to another developer and you've still got three full system designs, a map of your operation, and a HIPAA read.
Why Me, and What Happens Next
Banji referred you to me for a reason. For River Oaks I built a HIPAA-compliant system on self-hosted infrastructure that reads insurance documents, tracks approvals and denials, and auto-reconciles roughly 100 claims a week into QuickBooks. It saves him an estimated $30,000 to $40,000 a year in labor alone, before the denial recovery. Your billing and reconciliation work is a close cousin of that, and the intake side is the kind of front-of-funnel build I'm doing for another client right now across both web chat and email.
I came up running operations for a $35M+ D2C portfolio, so I read a business as an operator before a technologist. I'm not the cheapest automation hire you'll find. I'm the one who maps the whole board before touching a single build, so the thing that gets built is the right thing and it works the first time. The cheap version of this hands you a generic AI checklist and burns your runway on the wrong priority.
Next steps
If the signal's there, let's get the kickoff on the calendar this week so this doesn't slide into next month.